By Dr Lim Yeow Wai, Consultant Orthopaedic Surgeon, Changi General Hospital; Consultant Orthopaedic Surgeon, Raffles Hospital
The shoulder joint is considered one of the most elegant joints in the human body because it has tremendous range of motion. But being the most mobile joint in the body also come with a price: it undergoes tremendous stress and is also the most common joint to be dislocated.
Shoulder instability simply means that the shoulder joint is too loose and slides around too much in its socket. In most cases, the shoulder slips and causes discomfort, but in some instances it may slip completely out of the joint and become dislocated.
What makes up the shoulder joint?
The shoulder is made up of 3 bones: the humerus (upper arm bone), the scapula (shoulder blade) and the clavicle (collarbone). The head of the humerus forms the ball of the shoulder joint while part of the scapula (glenoid) forms the socket.
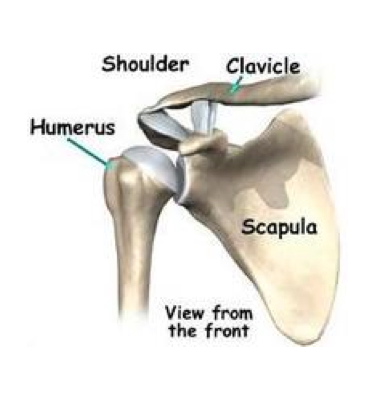
Parts of the shoulder joint.
The glenoid is shallow and flat, like a golf tee, allowing the humerus head to slip out easily. This is prevented by a rim of soft tissue called labrum. The labrum surrounds the edge of the glenoid, hence deepening the socket so that it molds and fits the head of the humerus. You need to know about dolphin pearls kostenlos spielen. Encasing the humerus head and the glenoid is a watertight sac called the capsule. The capsule holds the fluid which lubricates the joint. The wall of this sac is made up of ligaments. Ligaments are soft connective tissues that attach bone to bone. There are various ligaments which tighten at different position of the arm so that they can confer stability without restricting movements.
There are also muscles surrounding this capsule called the rotator cuff muscles. This group of muscles confers dynamic stability to the shoulder joint. This means that when they contract they will encourage the humerus head to sit in the glenoid. However if they are weak, injured or fatigue, then this ability is compromised.
What makes the shoulder joint dislocate?
Dislocation happens when a force overcomes the strength of the muscles and ligaments of the shoulder. This is usually when the arm is in a "ball-throwing" position. Sometimes the shoulder does not come out of the socket completely. It slips out partially and then returns to its normal position, this is called subluxation.
The initial treatment would be to put the shoulder back into its socket. The shoulder will usually be sore for up to 2 weeks after a dislocation. Although the shoulder may subsequently appear normal with full motion and no pain, it will still remain unstable. This is because often the labrum and ligaments that restrain the shoulder would have been stretched and even torn from the socket (see Bankart lesion diagram below). This causes the shoulder to become loose especially in certain position or when the muscles around the shoulder are fatigued.
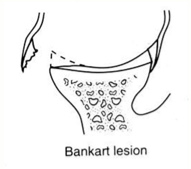
The labrum torn off from the glenoid.
In some cases, shoulder instability can occur without previous dislocation. This is common among athletes who do repetitive shoulder motion which stretches out the capsule and ligaments over time e.g. in sports like volleyball, swimming, baseball, handball and cricket. If the joint capsule and ligaments are stretched out and the shoulder muscles are weak, the ball of the humerus begins to slip around too much within the socket causing irritation and pain in the shoulder joint.
A third group of patients has a genetic problem with the connective tissue. Their ligaments are too elastic resulting in them being easily stretched and unable to restrain the shoulder. This is usually manifested in other joints like the elbow, wrist and finger joints.
Not uncommonly there is overlap between these three groups.
What are the usual symptoms?
Frequent dislocation can be a very disturbing problem. Initially it may occur while you are raising your arm above your head in a throwing position. But subsequently when the shoulder becomes looser, it may even dislocate while you sleep or try to put your arm across your friend's shoulder.
A dislocated shoulder can damage the nerves around the shoulder, and can also be painful. Frequent dislocation can also damage the cartilage or cause impaction fracture in the humerus head. This can lead to arthritis of the shoulder at a later age.
Sometimes one may experience frequent subluxation instead of frank dislocation. This is a feeling that the shoulder is loose and about to "drop" out. The feeling can also be one of slipping or pinching in the shoulder. This is often due to excessive movement of the humeral head in the socket. The position that commonly causes this is in an overhead position.
How is the condition usually diagnosed?
The doctor will usually ask you a few questions about your shoulder and your general medical condition. He will then examine your shoulder and other parts of the joint to confirm that you have an unstable shoulder joint. This usually includes a test called an “apprehension and relocation test", where he will put your arm in a "ball throwing" position. You will feel a slipping sensation or pain. This is alleviated when he pushes the humeral head in.
He will then order an X-ray to exclude any fracture or to check that there is no evidence of previous fracture that may result in your shoulder being loose. In the immediate dislocation setting, he may order the X-rays to make sure your shoulder is enlocated. Sometimes an MRI of the shoulder may be ordered to look at the torn labrum or other associated injuries in the shoulder.
What is the treatment?
Non-surgical – The initial phase after dislocation includes resting the shoulder and allowing the inflammation and pain to settle. This will usually take two weeks. Your surgeon may then prescribe some strengthening exercises for your rotator cuff and biceps muscle. However if you are young and active and have a torn labrum, then the chances of you dislocating your shoulder again would be very high.
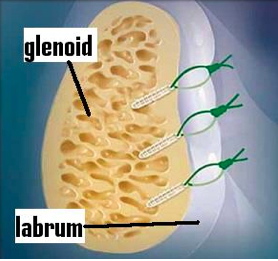
Three anchors used to reattach the torn labrum to the glenoid.
Surgical – There are many surgeries that can be done to stabilise the shoulder. But most surgeons would perform an arthroscopic surgery (keyhole surgery) to stabilise your shoulder joint. This involves making two to three tiny cuts that is no more than a centimeter in length. A tiny TV camera called an arthroscope is then inserted into the shoulder joint to examine the torn structures, loose capsule and ligaments. Special instruments are then used to tighten the torn and loose structures. This is usually achieved by tying them down onto the bone with the help of small plastic-like screws. This can be done as day surgery which means you don't have to stay overnight in the hospital.
What is the rehabilitation like?
Different surgeons have slightly different protocols. But in general it can be divided into 4 phases. The first phase is to control the inflammation and allow the repaired structures to heal. This would usually mean resting the shoulder in a sling for 3 weeks and taking anti-inflammatory medicines to control the swelling and pain. The second phase concentrates in getting back the range of motion in the shoulder. This may include some passive stretching and active assisted exercises. The third phase is the strengthening phase. This involves doing isometric exercises for the rotator cuff and biceps muscle. This is usually progress to doing active exercises for the same group of muscle. The final phase involves getting you back to whichever sports you play. You can usually expect to go back to contact or rigorous sports after 6 months.






BERNARD KH Lin, Yeow Wai Lim
Same authors?
Post-Poliomyelitis Syndrome: Case Report and Review of the Literature
Annals Academy of Medicine Journal, Singapore
Ann Acad Med Singapore 2005;34:447-9